.jpg)
Here is something worth sitting with before we go any further.
In most LGBTQ+ spaces, disability is an afterthought. Community events are often inaccessible. Resources assume verbal fluency and neurotypical processing. The faces centered in Pride campaigns rarely include people with intellectual disabilities.
In most disability spaces, sexual orientation and gender identity go almost entirely unaddressed. Staff may assume that individuals with IDD don’t have these identities — or may treat the topic as too complicated, too sensitive, or simply not relevant to their care.
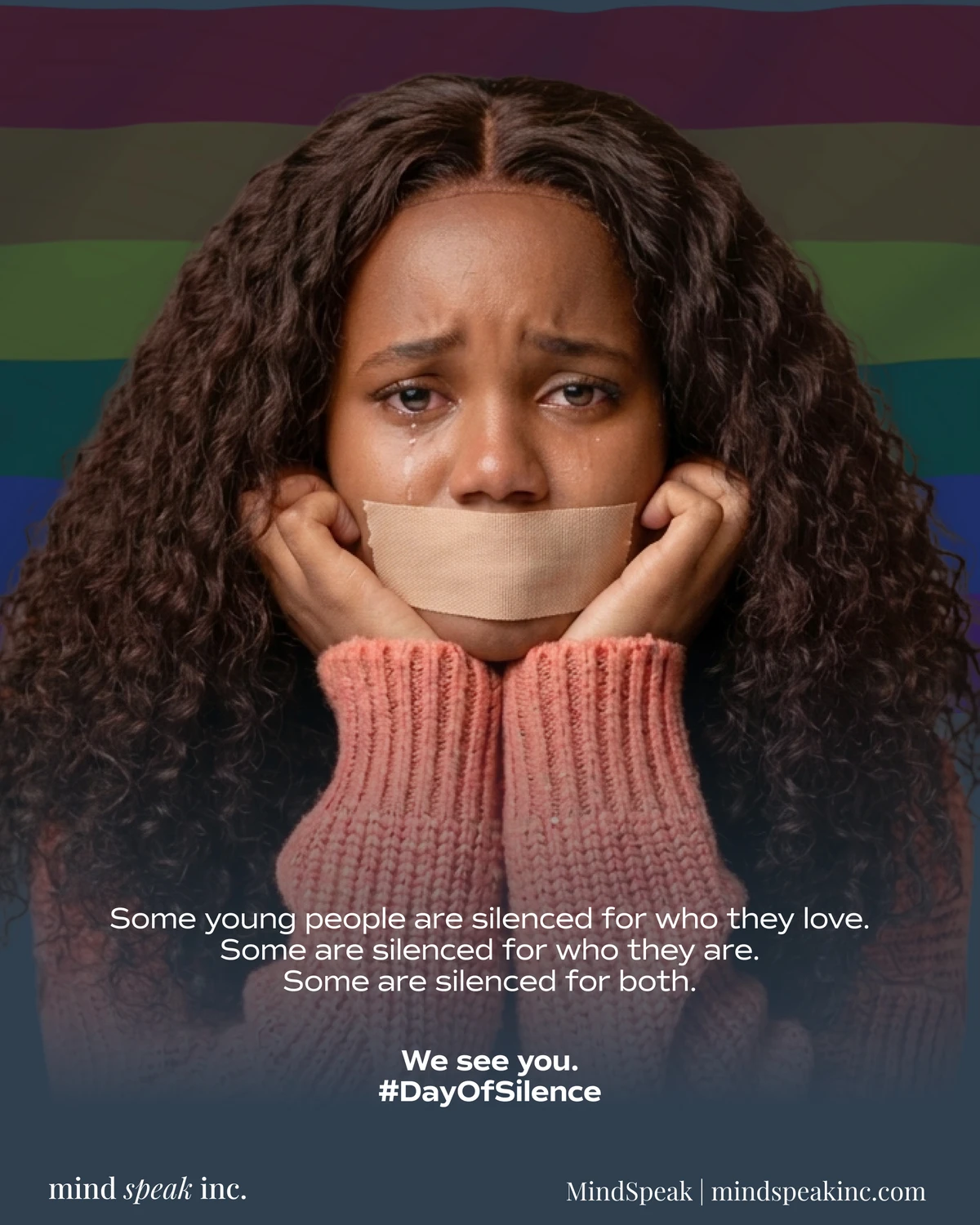
For someone who lives inside both identities at the same time, this double invisibility isn’t a theory. It’s Tuesday.
This is the experience of LGBTQ+ individuals with intellectual and developmental disabilities: fully belonging to two communities, and fully seen by neither. Understanding this intersection — and learning to support people across it — is not a niche concern. It is a matter of dignity, mental health, and basic human recognition.
The Double Invisibility Problem
Research estimates that between 8 and 13 percent of individuals with IDD identify as LGBTQ+, with many researchers noting that this is likely an undercount. Self-identification requires both the language and the safety to name one’s own experience — two things that are frequently withheld from people with IDD.
Yet these individuals exist. They have identities. They have emotional lives shaped by the same forces that shape everyone else’s: family response, community belonging, access to affirming relationships, and the experience — or lack — of being truly seen.
When neither their disability community nor their LGBTQ+ community holds space for their whole self, the result is compounded isolation. Not the ordinary loneliness of feeling different, but the more corrosive experience of having no space anywhere that reflects who you fully are.
This matters enormously for mental health. And it calls for something more than good intentions.

What the Research Tells Us
LGBTQ+ individuals already face significantly elevated rates of depression, anxiety, and suicidal ideation compared to their straight, cisgender peers — not because of their identities, but because of the environments those identities must navigate. Discrimination, family rejection, lack of affirming care, and social exclusion are the drivers.
Individuals with IDD, separately, also experience higher rates of mental health conditions. The reasons are different but overlapping: communication barriers, histories of trauma, limited autonomy, and a mental health system not always equipped to meet their needs.
When these two populations overlap, the risks compound. LGBTQ+ individuals with IDD may face family non-acceptance of both their disability and their identity. They may have limited access to age-appropriate sexuality education. They may be more vulnerable to exploitation and abuse. And they may have no affirming provider who holds competency in both areas simultaneously.
The protective factor is clear in the research as well: affirming relationships, environments that honor the full self, and access to knowledgeable support dramatically reduce mental health risk. The absence of these things is not neutral. It causes measurable harm.
What Families and Caregivers Often Get Wrong
The most common error is silence — treating identity as a topic that doesn’t apply, doesn’t need to be addressed, or will go away on its own.
Many families and caregivers hold an unexamined assumption that individuals with IDD don’t experience sexual orientation or gender identity in meaningful ways. This assumption is not supported by evidence. It is, however, deeply infantilizing. It removes the person’s inner life from consideration and treats their humanity as conditional on cognitive profile.
A related misstep is assuming that if the person has not explicitly named an identity, no identity exists. For individuals who have never had language for their experience — who have never seen themselves represented, never been offered affirming conversation, never been given permission to explore — silence is not absence. It is often suppression.
Families and direct support staff are in a powerful position here. When they create space — through language, through modeling, through the casual and consistent inclusion of LGBTQ+ representation in conversation — they signal safety. And safety is what makes self-expression possible.
When they avoid the topic, redirect it, or treat it as inappropriate, they signal the opposite. The person learns that this part of themselves is not welcome. That lesson compounds over time.

What Affirming Support Actually Looks Like
Affirmation is not a philosophy. It is a practice, and it shows up in specific, observable actions.
It begins with language. Using correct pronouns and chosen names — consistently, not just when it feels convenient — is a baseline, not an advanced skill. For individuals who have disclosed an identity or preference, honoring that in every interaction communicates that their self-knowledge is real and respected.
It extends into care planning. Person-centered plans, intake forms, and residential guidelines should include identity-affirming language and be regularly revisited. A plan developed five years ago may not reflect who someone is today.
It requires training that doesn’t silo. A staff member trained in IDD care but not in LGBTQ+ affirmation is only partially equipped. The same is true in reverse. Working with LGBTQ+ individuals with IDD requires both — not as separate modules, but as integrated competencies that shape how care is delivered every day.
It means connecting individuals to the community. LGBTQ+ peer spaces that are physically and communicatively accessible, that explicitly welcome people with disabilities, offer something that individual therapy cannot: the experience of belonging to a group that reflects your identity.
And it means seeking mental health providers who hold both competencies simultaneously — who can address identity alongside disability, and who understand that both are real, both matter, and neither can be treated in isolation from the other.
A few practical steps: - Never assume identity — create consistent, low-pressure space for self-expression at every age and stage - Audit the language in your care environment: are intake forms, care plans, and daily conversations identity-inclusive? - Train staff on both IDD-informed care and LGBTQ+ affirmation as integrated, not separate, skills - Connect individuals to LGBTQ+ peer communities that are accessible and explicitly disability-welcoming - Seek mental health providers trained in both areas — and ask about this directly when making referrals
Belonging Is Not Optional
Identity is not a complication in someone’s care plan. It is the person.
When an individual with IDD is also LGBTQ+, supporting their mental health means supporting all of who they are — not the disability piece this week and the identity piece when it becomes impossible to ignore. The two are not separate. They are woven together in the daily experience of being this specific person, in this specific body, navigating this specific world.
Pride Month is a meaningful time to name this. But the work of affirming LGBTQ+ individuals with IDD is a year-round commitment — in the language we use, the spaces we create, the providers we seek, and the assumptions we are willing to examine.
Every person deserves to be seen. Fully. Without exception.